Medical Researchers Examine Broad Spectrum of Coal Mine Dust Lung Diseases
Two researchers with the National Institute for Occupational Safety and Health’s Division of Respiratory Disease Studies have conducted a literature review concerning the lung diseases related to coal mine dust exposure. In order to improve clinicians’ abilities to better diagnose these diseases and recognize their association with work in coal mining, the researchers provide an overview of the literature related to the spectrum of diseases that are now referred to as Coal Mine Dust Lung Disease (CMDLD).
As the researchers point out, “A source of confusion around the term ‘CWP’ [Coal Workers’ Pneumoconiosis] is that in the United States, it has different meanings in clinical and statutory/legal settings.” The new term CMDLD is therefore used to describe the spectrum of lung diseases associated with exposure to coal dust. These include Coal Workers’ Pneumoconiosis (both simple pneumoconiosis and its severe form, Progressive Massive Fibrosis, or PMF), silicosis, mixed dust pneumoconiosis, dust-related diffuse fibrosis, and chronic obstructive pulmonary disease (COPD).
The authors establish a few key facts about the current state of CMDLD. Among them:
- 7% of long-tenured miners have Coal Workers’ Pneumoconiosis (CWP)
- 13.1% of actively working underground miners have lung function impairment
- The mean age of miners suffering from Progressive Massive Fibrosis (PMF) is 52.6 years
- The average years of potential life loss (YPLL) is 8.2 among decedents
- An association between disease prevalence and small mine size has been established
- Miners from Central Appalachia have substantially higher rates of CWP (3.7%) and PMF (1.2%) than miners from other parts of the country
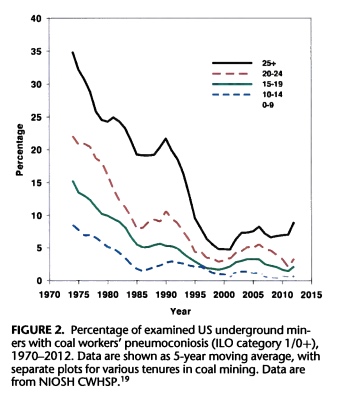
- Since 2000, rates of CWP have increased in incidence and severity (see figure 2, below)

The researchers also take note of CMDLD trends among surface miners:
“As already noted, the CWHSP [Coal Workers’ Health Surveillance Program] has previously been limited to underground coal miners. Thus, less data exists documenting the burden of pneumoconiosis in US surface miners. Still, it is well known that surface miners are at risk for pneumoconiosis. In 1983, a sentinel case of acute silicosis was reported in a surface coal mine driller. The case report included reanalysis of surveillance conducted in US surface coal miners in the early 1970s showing that drill crew workers were at significantly increased risk for pneumoconiosis relative to other surface coal miners. Medical examinations of surface coal miners in Pennsylvania conducted in 1984 and 1985 documented radiographic evidence of pneumoconiosis in 4.5% of men with no history of dusty work other than surface coal mining.”
The diseases associated with CMDLD have different pathological signatures, and require different medical procedures for diagnosis. “Classic patterns” of simple and complicated pneumoconiosis are rounded opacities, usually in the upper vertical zone of the lungs. The predominantly lower-zone, irregular small opacities that are synonymous with interstitial lung disease are best identified using high-resolution CT imaging. As the report explains, “In recent years, the United States has seen an increasing burden of CMDLD-interstitial diseases, particularly in the central Appalachian region.”
The review explains that dust-related diffusive fibrosis (DDF) occurs much more frequently in long-tenured coal miners than idiopathic pulmonary fibrosis does in the general population. (Idiopathic pulmonary fibrosis is a chronic and ultimately fatal disease characterized by a progressive decline in lung function. The term ‘idiopathic‘ is used because the cause of pulmonary fibrosis is still unknown.) Accordingly, it is more likely that a miner diagnosed with IPF actually has DDF, a form of CMDLD.
Because CMDLD can only be treated symptomatically, the review emphasizes that prevention is critical.
We’ve embedded the review below.
Laney and Weissman – Respiratory Disease Caused by Coal Mine Dust.pdf by trayclc