Lung Transplants for Miners with Black Lung: New Research Shows More Transplants Being Done, Most Transplants Being Paid for by Public Dollars NOT by the Coal Industry

Image from Penn Medicine’s Penn Transplant Institute
I have been slow to post about a recent piece of medical research about the increasing rates of lung transplants for miners with black lung.
Initially, I wasn’t sure exactly what to make of the article, so I was very glad to see that public health expert Dr. Celeste Monforton wrote a terrific piece on The Pump Handle blog about it.
My goal here is to provide access to these pieces in case you missed them and then to add a few of my own thoughts after thinking about these issues for a couple weeks.
The Medical Research on Lung Transplantation Among Coal Miners
On January 4th, the American Journal of Industrial Medicine published online an article titled “Lung Transplantation Is Increasingly Common Among Patients with Coal Workers’ Pneumoconiosis” (embedded below as a downloadable pdf). The article, written by NIOSH researchers Dr. David J. Blackley, Dr. Cara N. Halldin, Dr. Kristin J. Commings, and Dr. A. Scott Laney, examines trends in lung transplantations for patients with CWP or “unspecified” pneumoconiosis from 1996 to 2014. The purpose of this research was to see if and how the United States’ increasing black lung rate was affecting lung transplantation among coal miners.
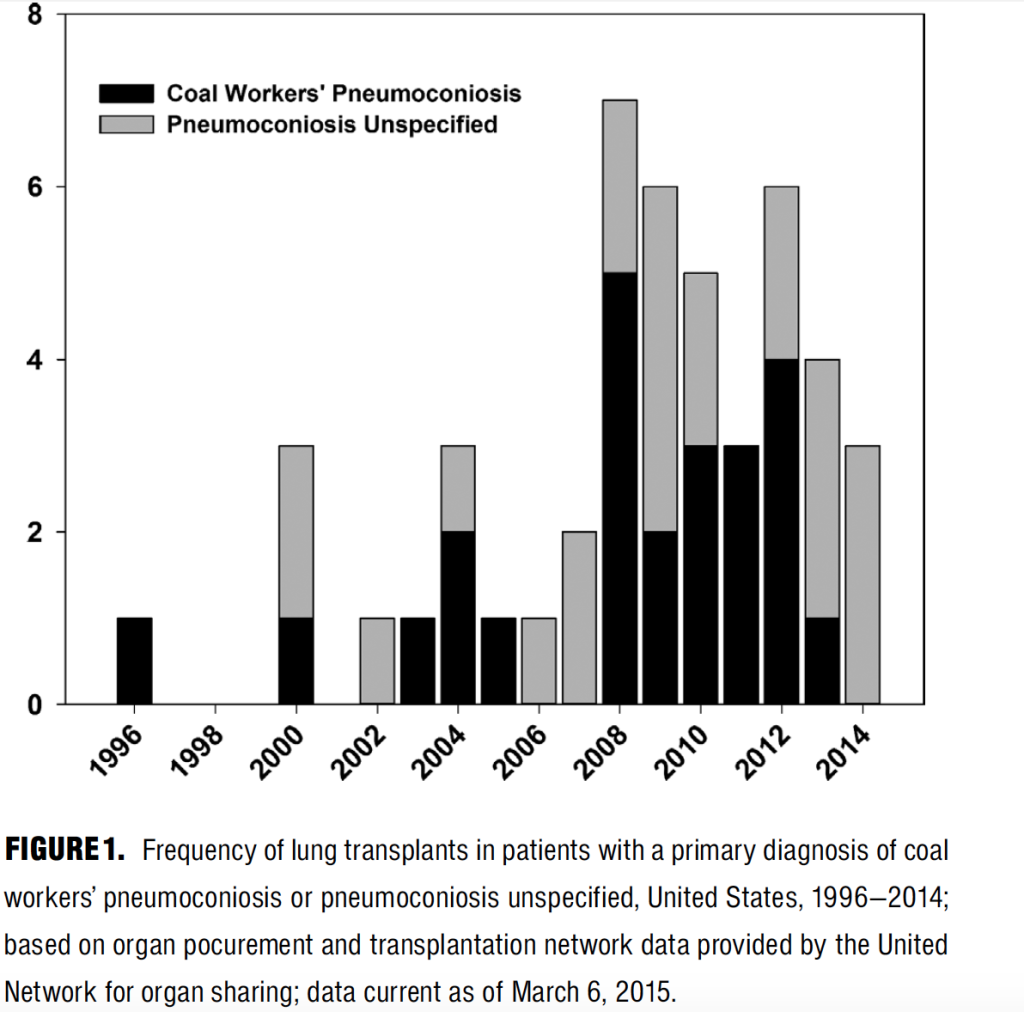
The article found that during the period, 47 individuals with CWP or unspecificied pneumoconiosis received lung transplants. Of the patients with unspecified pneumoconiosis, 19 of the 23 were from West Virginia, Virginia, Kentucky, or Pennsylvania—suggesting that most of the unspecified pneumoconiosis was likely found among coal miners. Even though the period covered 18 years, 72% of the transplants were performed in the last 7 years, a finding consistent with the recent resurgence of severe black lung.
The mean age of the individuals receiving transplantation was 56 years. The median post-transplant survival was 3.7 years.
The authors discussed the findings as follows:
Although transplants for CWP are relatively rare compared to the total number performed in the U.S., the procedure is becoming increasingly common, and its success with respect to survival is not entirely clear.
. . .
These results add to a growing body of evidence pointing to increased severity of coal mine dust lung disease in the U.S. and highlight the mounting consequences of this ongoing epidemic. A lung transplant for end-stage CWP is an extreme intervention, but in the absence of proven curative treatments, U.S. coal miners will continue to undergo the procedure. These transplants reflect the use of a scarce resource for an entirely preventable disease, and highlight the need for enhanced efforts to reduce coal mine dust exposures.
Dr. Monforton’s Response
I suggest that you pause at this point and read the entirety of Dr. Celeste Monforton’s post—titled “Who’s paying the cost of lung transplants for work-related lung diseases?“—on The Pump Handle blog (a multiauthor blog on ScienceBlogs.com that intends to serve as a “water cooler for the public health crowd”).
Dr. Monforton’s piece focuses on the substantial financial cost of the transplants—an average of $1.04 million—and asks who is paying. Dr. Monforton points out that it is troubling that only 34% were being paid for by private insurance and that the rest were being paid for by Medicare (30%) or “other government insurance schemes” (36%)—e.g., black lung benefits covered by the Department of Labor’s Black Lung Disability Trust Fund. As she explains, the use of Medicare and Trust Fund dollars for these expensive procedures is troubling and may be the result of the coal industry’s efforts to challenge the procedures in individual miners’ cases.
Dr. Monforton then notes that the industry is also fighting MSHA’s new rule that would lower respirable coal-mine dust and concludes
I think their money would be better spent on controlling respirable coal mine dust than on lawyers’ fees. But if coal companies aren’t held accountable for the full cost of black lung disease, including $1 million lung transplants, why would they?
My Response
The NIOSH research is interesting but sobering. The fact that stood out the most to me was the young age (average 56 years old) of the individuals getting the transplants and the fact that the median survival rate was 3.7 years. This means that half of these working-age men did not live much more than 3 1/2 years after getting their new lungs.
As an attorney who helps miners get black lung benefits, I hope that the medical benefits will help my clients enjoy and extend their lives. This grim statistic was a reminder that black lung truly is incurable and then even the most drastic remedies have a limited likelihood of success. With that being said, there are individuals that this makes a big difference for. My firm, Appalachian Citizens’ Law Center, has helped a miner use his black lung benefits for a lung transplant that continues to improve the miners’ life.
Dr. Monforton’s points about the importance of ensuring that the industry bears the full costs of the diseases that it creates is important and her argument that the industry challenges lung transplantations in individuals cases is true. For just one public example, remember the case of Robert Bailey who testified before a Senate subcommittee while waiting on this transplant (see previous post here).
For me, the core takeaway from all of this is that black lung is devastatingly dangerous and devastatingly expensive and that the only reasonable solution is to prevent the disease. Our society spent approximately $47 million dollars (much of it taxpayer dollars) to give these individuals a few more years of life. Those years were doubtlessly immeasurably valuable, but what if that money had been spent preventing the miners’ exposure to dust on the front end. Controlling coal-mine dust is expensive, but so is failing to. And when our society fails to prevent black lung, then we not only have to pay, but also the miners and their families have to suffer needlessly.
As the science around lung transplantation progresses, we should have better results in the future. But we should also work to ensure that it is less needed and that the costs are borne by the people who can prevent black lung.
Lung Transplantation is Increasingly Common Among Patients with Coal Workers' Pneumoconiosis
4 Responses to “Lung Transplants for Miners with Black Lung: New Research Shows More Transplants Being Done, Most Transplants Being Paid for by Public Dollars NOT by the Coal Industry”
How is CWP and non-specified pneumoconiosis specified. In black lung one may talk about Clinical and legal pneumoconiosis . Clinical was often defined as with a positive xray . Clinical was disease diagnosed without a positive film . This may a problem as it confuses an ability to diagnose CWP without a positive xray and other lung disease caused by coal mine dust exposure. So in this report how is CWP being specified vs pneumoconiosis non specified ??
Very good question! It’s not clear from the study how CWP vs. unspecified pneumoconiosis were defined. My guess is that it probably depended a lot on how the physicians who were involved with each transplant decided to code the disease and that the pneumoconiosis in this study would be “clinical pneumoconiosis” rather than “legal pneumoconiosis.” If you want better information on this, I’d suggest getting in touch with the study’s corresponding author, David Blackley, whose contact info is at the bottom of the first page of the article. If you find out, let us know!
[…] The host interviews a retired coal miner Howard Cook from Letcher County, Kentucky with complicated black lung and epidemiologist Dr. David Blackley from NIOSH who has done research into the resurgence of black lung (for examples of Dr. Blackley’s research, see here, here, here, and here). […]
[…] by the American Journal of Industrial Medicine on May 6, 2018. The article is a continuation of research from 2015 showing increases in the number of coal miners who need lung transplants. The recent data shows […]
Comments are closed.